
byJohns Hopkins University School of Medicine
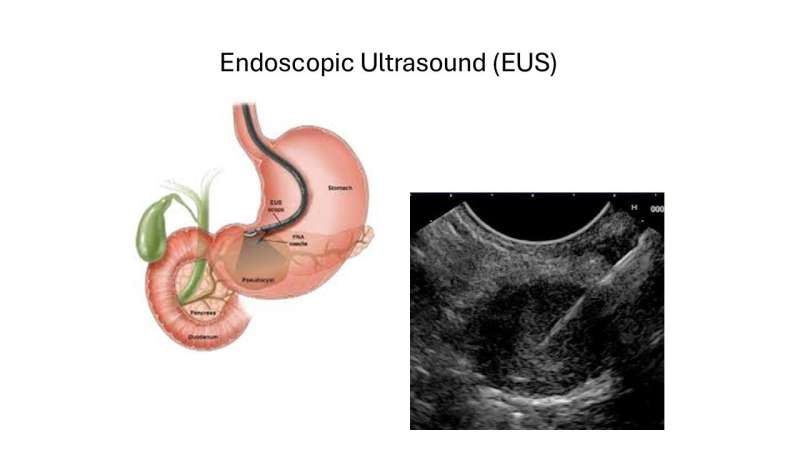
The image shows an ultrasound endoscope in the stomach imaging the pancreas (left picture) and corresponding small pancreatic cancer that is undergoing fine needle biopsy under endoscopic ultrasound (EUS) guidance. EUS is one of the main tools used for surveillance of high risk individuals and it can detected and diagnose asymptomatic tumors in the pancreas during a routine surveillance visit. Credit: Marcia Canto
Pancreatic ductal adenocarcinoma is projected to become the second-leading cause of cancer death in the United States by 2030, according to the National Institutes of Health (NIH). The International Cancer of the Pancreas Screening (CAPS) Consortium, the American Society for Gastrointestinal Endoscopy, and the National Comprehensive Cancer Network currently recommend surveillance for high-risk individuals, including individuals with multiple immediate blood relatives who have had pancreatic cancer as well as those identified as having a genetic predisposition.
In a new Johns Hopkins Medicine study, researchers found mild dilatation, or enlargement, of the pancreatic duct is a cancer risk factor that should be monitored in high-risk individuals.The studywas published inGastro Hep Advancesin November 2025.
"We are identifying pancreas duct dilatation as an early sign of pancreatic cancer in high-risk individuals even when there is no visible mass. This finding may lead to better survival if cancers are detected early," says Marcia Irene Canto, M.D., M.H.S., a professor of medicine and oncology at the Johns Hopkins University School of Medicine.
Canto says this investigation is part of the CAPS Study, an ongoing, long-term, prospective cohort study of high-risk individuals with a familial orgenetic predispositionfor developing pancreatic adenocarcinoma. The study was initiated in 1998. Johns Hopkins Kimmel Cancer is one of the foremost leaders in pancreatic research andpatient care.
In this research, Johns Hopkins Medicine experts evaluated the outcomes of a CAPS cohort of 641 high-risk individuals. During routine surveillance withendoscopic ultrasoundand MRI, the researchers measured the participants' pancreatic ducts and found that in patients with a duct diameter greater than 4 millimeters, the chances of developing either high-grade dysplasia or cancer increased. Moreover, participants with widened pancreatic ducts were more likely to develop cancer early.
Of the 641 participants evaluated, 97 showed enlargement without evidence of an obstructing mass lesion; 10 of whom were diagnosed with neoplastic progression within a median of two years after dilatation was first detected. The cumulative probability of pancreatic cancer with baseline duct widening was 16% at five years and 26% at 10 years. Participants were 2.6 times more likely to progress to acancer diagnosis, particularly those with more than three pancreatic cysts during surveillance.
"By identifying this risk factor early, we were able to intervene more quickly," says Canto. "The intervention would be to either operate or do much more frequent imaging. It was remarkable how even with the best imaging technology, apancreatic cancermass may not be visible even when it is causing structural changes in the gland. We have an opportunity to do better."
Canto says this early warning sign of pancreatic duct dilation could be a valuable finding identifiable with other kinds of diagnostic imaging, such as CT performed for unrelated health issues like kidney stones or abdominal pain.
"The dilatation is a red flag [in high-risk patients]," Canto says. "Providers should be aware that it is something that needs to be addressed right away."
Canto says the next step in the research is usingartificial intelligenceto analyze imaging and clinical information to make more specific and accurate predictions of risk.
More information: Elizabeth Abou Diwan et al, Mild Dilatation of the Main Pancreatic Duct Is a Risk Factor for Progression to Pancreatic Cancer in High-Risk Individuals, Gastro Hep Advances (2025). DOI: 10.1016/j.gastha.2025.100802
Provided by Johns Hopkins University School of Medicine




Post comments