
byJustin Jackson, Medical Xpress
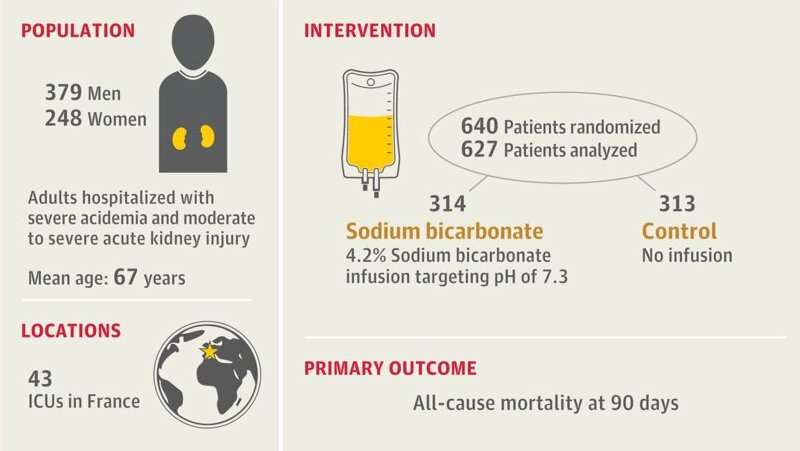
Visual abstract. Credit:JAMA(2025). DOI: 10.1001/jama.2025.20231
Montpellier University Hospital leads a 43-center French effort that reports no reduction in day 90 all-cause mortality with sodium bicarbonate infusion for critically ill adults with severe metabolic acidemia and moderate to severe acute kidney injury.
Severe metabolic acidemia (acidic blood) has been linked to impaired cardiac contractility, arrhythmias, pulmonary vasoconstriction, systemic vasodilation, alteredkidneyblood flow, cerebral edema, and diaphragmatic dysfunction.
Common etiologies in critical illness include hyperchloremic acidosis, lactate accumulation, and endogenous anion accumulation duringacute kidney injury.
In the human body, carbon dioxide combines with water viacarbonic anhydraseand forms carbonic acid, which dissociates into a hydrogen ion and bicarbonate. Early 20th century investigators described metabolic bicarbonate as an "alkaline reserve," naturally buffering the body to keep a healthy acid-base balance.
Sodium bicarbonate entered acute care protocols in the 1950s as a staple of cardiopulmonary resuscitation (CPR) guidance. Skepticism grew across the 1980s and beyond as routine dosing failed to show outcome advantages and reports raised concerns about potential harms.
Modern evidence, including recent trials, has coincided with removal of routine bicarbonate use from American Heart Association CPR guidelines, with use retained for select cases of severe acidosis.
Prior work by the Montpellier team on bicarbonate outcomes did not show an overall benefit from sodium bicarbonate, though an acute kidney injury intervention suggested benefit, leaving open the possibility that it still might be of benefit under specific conditions.
In the study, "Sodium Bicarbonate for Severe Metabolic Acidemia and Acute Kidney Injury: The BICARICU-2 Randomized Clinical Trial,"publishedinJAMA, researchers conducted an open-label, investigator-initiated, multicenter randomized clinical trial to determine whether sodium bicarbonate infusion reduces day 90 all-cause mortality after severe metabolic acidemia with moderate to severe acute kidney injury in critically ill adults.
Adults in 43 French intensive care units were screened with 627 analyzed for the primary outcomes. Participants were assigned 1:1 to intravenous 4.2% sodium bicarbonate or nosodium bicarbonate. Each infusion was 125 to 250 mL over 30 minutes, with a maximum of 1,000 mL in 24 hours and blood gas checks after each infusion. Indications for kidney replacement therapy were standardized in both groups.
The primary outcome was day 90 all-cause mortality. Secondary outcomes included day 28 and day 180 mortality, use of kidney replacement therapy, vasopressors, or invasive mechanical ventilation, lengths of stay, ICU-acquired infections, fluid balance, day seven Sequential [Sepsis-related] Organ Failure Assessment score, and major adverse kidney events on day 90.
Day 90 all-cause mortality reached 62.1% in the bicarbonate group and 61.7% in the control group, yielding an absolute difference of 0.4, a statistically non-significant difference (P=.91). Time-to-event analysis showed a hazard ratio for death of 0.97, also non-significant (P=.78).
Analyses adjusted for randomization strata and additional modeling, including inverse probability weighting, did not show evidence of a group effect. Subgroup analyses across randomization strata and exploratory categories also did not show evidence of disparity.
Kidney replacement therapy occurred in 35% of the bicarbonate group and 50% of controls, an absolute difference of −15.5%. Median time to kidney replacement therapy initiation measured 30.9 hours in the bicarbonate group and 15.5 hours in controls. The hazard ratio for initiation through day 28 was 0.59. ICU-acquired bloodstream infections occurred in 4% of the bicarbonate group and 9% of controls, possibly related to lower kidney replacement therapy.
Other secondary outcomes did not show evidence of a group effect, including vasopressor or invasive mechanical ventilation use, Sequential [Sepsis-related] Organ Failure Assessment scores, or lengths of stay. Adverse events did not differ by group.
Sodium bicarbonate therapy did not affect day 90 mortality in patients with severe metabolic acidemia (pH ≤7.20) and moderate to severe acute kidney injury.
Less frequent kidney replacement therapy use in thebicarbonategroup and lower bloodstream infections illustrated significantly better outcomes.
© 2025 Science X Network
More information: Boris Jung et al, Sodium Bicarbonate for Severe Metabolic Acidemia and Acute Kidney Injury, JAMA (2025). DOI: 10.1001/jama.2025.20231 Prit Kusirisin et al, Sodium Bicarbonate in Severe Acidemia and Acute Kidney Injury—Turning the Tide or Chasing a Myth?, JAMA (2025). DOI: 10.1001/jama.2025.20457 Journal information: Journal of the American Medical Association





Post comments